Arthroscopy is a common surgical procedure in which a joint is accessed through a small camera (arthroscope) and specially designed tools. Knee arthroscopy gives the surgeon a clear view of the interior of the joint, useful for the diagnosis and treatment of various conditions.
Technological advances have led to high-resolution screens and cameras, making arthroscopy a very effective knee replacement tool. According to the American Society of Sports Medicine, more than 4 million knee arthroplasties is performed worldwide each year.
DESCRIPTION
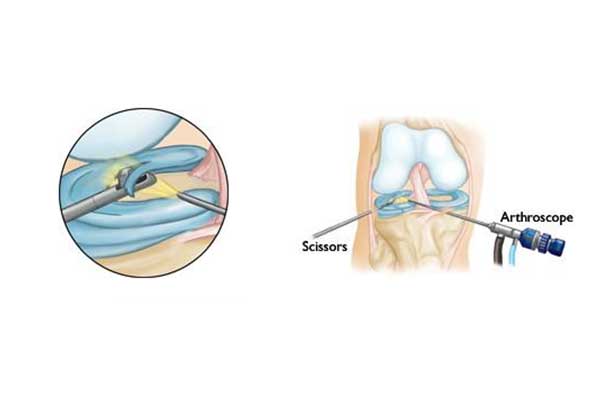
Arthroscopy is performed with very small incisions through which the orthopedist inserts the arthroscope (a small instrument with the size of a pencil) into the knee joint. The arthroscope sends the image to a television screen in which the surgeon can view the structures of the knee in great detail. The orthopedist can use arthroscopy to repair or remove damaged tissues and to do so special tools are inserted through adjacent small incisions.
PREPARATION FOR SURGERY
Before knee arthroscopy, a thorough examination may be needed to identify health problems affecting the procedure. In addition, the orthopedist must be informed on any medications or supplements the patient takes. Preoperative testing includes blood tests and electrocardiogram (ECG).

SURGERY
In most knee arthroscopic procedures, the patient is discharged on the same day.
ARRIVAL: The patient is informed in detail by the hospital for the appointment. Usually, the patient should arrive at the hospital 1 to 2 hours before surgery, fasting from the previous night.
ANESTHESIA: When the patient arrives, the anesthesiologist visits him/her and discusses all available options on anesthesia (general, regional, local).
- In local anesthesia, the knee area is “numb”.
- In the peripheral anesthesia (dorsal or epidural) the body is anesthetized below the waist.
- In general anesthesia the patient is asleep.
The anesthesiologist helps the patient make the right decisions. If the patient undergoes local or regional anesthesia, he or she is able to monitor the operation on the display screen.

SURGICAL INTERVENTION
The Orthopedist makes specific and very small knee incisions. The joint is filled with sterile solution (saline) followed by a thorough washout. Thus, the surgeon can review the knee structures clearly and in great detail.
The first step is to diagnose or confirm the diagnosis. If treatment is needed after diagnosis, special tools are inserted through small incisions. These include special arthroscopic scissors, arthroscopic diathermy and the shaver (a special high energy reamer).
This part of the procedure usually lasts 30 minutes to one hour, as appropriate.
Knee arthroscopy is most commonly used in:
- Removal or restoration after meniscus rupture.
- Restoration after rupture of the anterior cruciate ligament.
- Scraping – removal of degenerated articular cartilage.
- Removal of loose bodies (bone or cartilage fragments).
- Removal of inflammatory articular tissue.
Finally, the small incisions are sutured with one or two stitches each and covered with a soft bandage. Depending on the case, the patient may return home on the same day or on the next day, always accompanied (as driving is contraindicated in the first 24 hours).

TREATMENT – RECOVERY
Recovery after knee arthroscopy is much faster than traditional open surgery. Nevertheless, it is important for the patient to follow the instructions of the Orthopedist during the postoperative period.

EDEMA
Improper limb position (leg up) and ice therapy can prevent edema for the first few days.
CARE OF THE INJURY AND THE BANDAGES
The patient is discharged with a bandage around the knee. The wound must be kept clean and dry. The surgeon will give instructions on when the patient may change the bandage or take a shower or bath. After a few days, the patient visits the surgeon to check his/her progress, clinical condition and to begin the post-operative treatment program.
CHARGING THE KNEE WITH LOADS
Most patients need crutches after surgery. The surgeon decides when it is safe for the patient to charge the operated leg. Any questions should be answered by the treating physician.
DRIVING
The treating physician based on the patient’s progress will allow the return to driving. This decision will depend on a number of factors, such as:
- The knee involved
- Whether it is automatic car or not
- The type of surgery
- The level of pain
- Whether or not and to what extent opioid painkillers are used
- The level of knee mobility
Under normal conditions, patients are able to drive 1 to 3 weeks after surgery.
MEDICATION
Your doctor prescribes analgesic medications to relieve pain after surgery. In addition, as appropriate, the doctor shall prescribe drugs such as aspirin or heparin (Low Molecular Weight Heparin) to reduce the risk of thrombosis.
KNEE STRENGTHENING EXERCISES
The patient should be exercised daily and on a regular basis for several weeks after surgery, focusing primarily on the operated knee. This will restore the range of motion and muscle strength around the joint. Postoperative mobilization and exercise will play an important role in the final result.
COMPLICATIONS
As with any surgery, some complications may occur in arthroscopies. They are rare and usually of minor importance.
Possible postoperative complications after knee arthroscopy include:
- Infection (surgical trauma infection)
- Thrombosis
- Hematoma (Hemarthrosis)
SYMPTOMS (“WARNING SIGNS”)
The patient should call the surgeon immediately, if he or she presents any of the following symptoms:
- Fever
- Shudder
- Persistent edema or redness in the knee
- Significant increase in pain level
- Swelling and pain in the legs (gastrocnemius)
RESULTS
The patient is able to return to his or her daily activities after 6 to 8 weeks, unless it is a cruciate ligament rupture repair. As far as sports activities are concerned, it may take a longer period of time, which will be decided by the surgeon.
If the patient’s profession involves heavy work, sick leave may be the choice of option. For safety reasons, the doctor will discuss with the patient a safe return to work.
The final clinical outcome of the surgery is largely determined by the knee injury. For example, if the articular cartilage is severely damaged, complete recovery is not possible. This can mean restricting activities and changing lifestyles.
