Shoulder Physiology
The shoulder is a complex of joints that includes:
The glenohumeral joint (head and glenoid cavity)
The scapulothoracic joint (the scapula moving in relation to the chest)
The acromioclavicular joint (the outer end of the clavicle connected to the acromion)
The sternoclavicular joint (the inner end of the clavicle connected to the sternum)

Rotator cuff disorders – Rotator cuff
General Information
The rotator cuff of the shoulder consists of 4 muscles that attach to the scapula and the humerus and form a petal around the humeral head and the glenoid cavity. These muscles help the head move in the glenoid cavity and compress and stabilize the head within the glenoid cavity by acting as a fulcrum during the rotational movements of the humerus.

The 4 rotator cuff muscles are the supraspinatus, the subscapularis, the infraspinatus, and the teres minor.
The rotator cuff muscles compress the head into the glenoid cavity during active shoulder movement.

The rotator cuffis involved in a variety of movements including liftof the upper extremity, inner rotation (moving the upper extremity towards the inner side of the body, thereby allowing you to place your hand behind your back), and outer rotation (moving the upper extremity towards the outer side of the body allowing you to place your hand behind your head).
What is the Impingement Syndrome?
The shoulder Impingement Syndrome is the mechanical compression of the rotator cuff (mainly the supraspinatus tendon and the infraspinatus tendon) on the acromion tip. This condition can lead to a rupture of the rotator cuff. The term “compression”, of course, is oversimplified. When the upper extremity is elevated in repeated activities, such as swimming, tennis or even at work, there may be irritation of the subacromial serous membrane, which we would characterize as a lubricant that interferes between therotator cuff and the acromion. If this layer of the subacromial serous membrane becomes inflamed and swollen due to injury, then it can be pressed between the rotator cuff and the acromion. Sometimes an osteophyte may be formed, which contributes to the deterioration of the impingement syndrome.
In some patients a large osteophyte may be an important part of the impingement syndrome, although this is relatively rare. If this is the case, however, this osteophyte is removed during arthroscopy using a specialized tool. Removal of this osteophyte, while also removing the inflamed membrane, increases the space for the rotator cuff movements to be unhindered. The part of the subacromial serous membrane that we have surgically removed is replaced by a new membrane.

What is the rupture of the rotator cuff (mainly of the supraspinatus tendon) and how it occurs?
The rotator cuff can be injured by repeated movements above the level of the head, a sudden injury or a combination of both. During our lives, our hand is repeatedly positioned above the level of the head so that the rotator cuff is likely to be irritated by compression on the acromion. The rotator cuffis inserted on the rim of the humerus around the humeral head.
If you have pain but not great weakness, then your tendon may be inflamed rather than cut (tendonitis). The membrane above the rotator cuff is called serous membrane and can also be inflamed. This is called bursitis. The combination of bursitis and tendon inflammation is called friction syndrome. When the tendon is torn, pain and weakness usually coexist. Another common symptom is nighttime pain that interferes with sleep and worsens when we sleep on the injured shoulder. The most common tendon to be ruptured is the supraspinatus, located at the top of the head and glenoid cavity.

In the following figure the supraspinatus tendon rupture is triangular in shape, but it may also vary in shape and size.

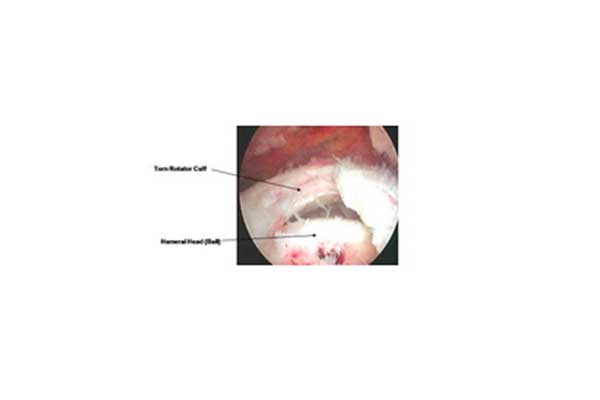
The arthroscopic appearance of the ruptures of the rotator cuff (the supraspinatus tendon) is depicted in the figure below.
The image on the magnetic resonance tomography (red arrow) of the supraspinatus tendon (yellow dotted line) is shown below.

Treatment of Friction Syndrome and Rotator Cuff Ruptures
The rotator cuff may be injured by repetitive movements of the upper limb above the level of the head, by a sudden injury or a combination of both. Initial treatment is usually conservative and in this way the symptoms usually ameliorate in the course of time, following an appropriate treatment plan.
Physiotherapy: A physiotherapy program by a qualified physiotherapist can improve your physical strength and reduce pain.
Anti-Inflammatory Drugs: Your doctor may prescribe medication to limit inflammation.
Cortisone injections: In some cases, cortisone injection is indicated. This will usually offer very good results in terms of pain. The benefits include a better night-time sleep and greater effectiveness of the physiotherapy program. Even if the injection provides only temporary relief from pain, it will help confirm the diagnosis.
Surgical Recovery: In most cases, surgical repair is performed arthroscopically, giving the patient the opportunity to return home on the same day.
Arthroscopic repair of the rotator cuff rupture is a common procedure, but it requires specialized training, not only for the tendon repair stage, but also for the correct judgment of how to repair the rupture.
The tendons that are subject to rupture are not normal, so the size of the tendon’s wear can vary. Sometimes there is a rupture in tendons that have a fine texture and not good quality. The quality of the tendon is of great importance for the period required for rehabilitation and the successful outcome of the surgery. Chronic ruptures generally have worse prognosis and this is exacerbated if there is a medical history of heavy smoking. The good quality of the tendon is linked with a thick and dense tendon with elasticity.
When supraspinatus or the infraspinatus muscle is atrophied and not sutured then the shoulder functionality is restored by another procedure called reverse total shoulder arthroplasty.
Post-surgery rehabilitation: After surgery the tendon is protected with a pillow, which acts as a splint for 4-6 weeks. A rehabilitation program should be commenced 6 weeks later, under the supervision of a qualified physiotherapist. Return to activities (sports or non-sports) is permitted within 4 months or slightly longer than the day of surgery. If the tendon is not repaired in the operating room, but only the inflamed serous membrane and the osteophytes are removed, then return to daily and sports activities is permitted within a few weeks.
Frequent asked questions
Question: Will my tendon heal if I do not undergo surgery?
Answer: Ruptured tendons are not normal and usually bear some degree of degeneration. So they are weaker than normal tendons. This can be a result of age, usage as well as other factors. Ruptured tendons do not heal on their own.
Question: Will I feel pain if I do not undergo surgery?
Answer: The pain may subside but the tendon will not heal. Studies have shown that in people who use their hands for work or sports activities, surgical repair of the tendon contributes to greater pain relief and better strength than non-surgical repair.
Question: Will I get worse if I do not undergo surgery?
Answer: Although many people do not experience any disability or pain in a chronic rotator cuff rupture, the tendon rupture may get larger over time. Some patients may even become more symptomatic. The underlying risk is that if the rupture becomes larger, it may be more difficult to repair in the future. In addition, the muscles that compose the rotator cuff, which adheres to the tendon, can become more atrophic (shrink and become smaller). Muscles also degenerate and become fattier and scarred compared to normal muscles. If this happens, the rotator cuff muscles will be less likely to contract as healthy muscles. Tendon restoration to previous levels may not be achieved at all, if the muscles become atrophic and have undergone fat infiltration and scarring. The length of time required for this is unknown, but animal studies have shown that it can be observed within 3-6 months after rupture, if the cause of the rupture is a traumatic event.
Question: What can I do pre-operatively to assist recovery post-operatively?
Answer: It is well known that smoking is associated with the development of rotator cuff ruptures and consequently such ruptures tend to become larger in people who smoke. In addition, smoking has been found to interact with tendon healing in animal studies. So if you smoke it would be best to quit smoking as soon as possible before going to the operating room and not to smoke throughout the recovery period. The use of anti-inflammatory drugs also interacts with the healing of the tendon, so such medicines should be avoided before and after surgical treatment.
Question: How fast will I recover after surgery and how soon can I play sports or lift weights?
Answer: Small tendon ruptures are usually immobilized on a splint for a period of 4 weeks postoperatively, while major ruptures are treated with 6 weeks of initial immobilization. The tendon healing thus allows the patient to lift the hand on a daily basis, but not yet to participate in sports activities. Strengthening is usually permitted within 3 months after surgery and complete return to sports activities is possible 4 months after surgery. Weight lifting and combat sports involving physical contact with athletes should be avoided for at least 6 months after surgery.
Question: When can I take a bath after surgery?
Answer: This is usually allowed 3 days after surgery as the relatively small incisions performed during arthroscopy are healed during this period of time. If a larger incision was required during surgery, then your surgeon will advise you not to wet the wound for a while. So, you should avoid wetting the affected area during showers.
Question: How functional will my shoulder be after surgery?
Answer: All patients differ in the quality of the repaired tendon and in the size of the ruptured tendon. Most patients experience significant improvement in pain and overall function. Over 90% of patients feel they have benefited from surgery when asked about it 1 year after surgery. The degree to which strength and endurance are regained depends largely on the quality of the tendon and on the completion of the healing process. In addition, the chronicity of the problem adversely affects the absolute capacity of the rotator cuff muscles to create a strong shoulder.
Question: What is the risk of getting worse after surgery?
Answer: The risk of complications after an arthroscopic restoration of rotator cuff ruptures is very small. There is an extremely rare possibility for an allergic reaction to anesthesia drugs. Surgical complications may include infection (<1%), and shoulder stiffness (<1%). Shoulder stiffness is known as a “frozen shoulder” and may be observed after any shoulder surgery. The etiology of a postoperative “frozen shoulder” is usually the body’s overreaction to the surgical stimulus, the inflammation and the scarring. This problem is usually resolved with a treatment plan, but the overall recovery period is longer than it would have been in case the complication had not occurred.
In rare cases a patient may experience more pain or less functionality or both after surgery, although there is no clear indication of exactly what the cause may be. This may be due to subtle changes in the mechanical function of the shoulder after surgery. This chance is well below 1%, according to our opinion and based on our experience.
Question: Is there a chance I may need to have an open surgery or all shoulder surgeries are arthroscopic?
Answer: Most rotator cuff ruptures can be treated with arthroscopic surgery. The indications for open surgery are usually related to the need to treat other parameters that may have been caused by a previous surgery. Such parameters can be deltoid injury, acromion fracture or chronic shoulder injuries.
