The tendons are strong structures of fibrous tissue that connect the bones to the muscles. The quadriceps tendon works with the muscles on the anterior surface of the thigh to extend the knee.
Small ruptures in the tendon make it difficult to walk and participate in daily activities. On the contrary, a major rupture in the quadriceps tendon is a serious injury that requires surgical treatment and subsequent physiotherapy to restore knee function.
These ruptures are not common. Most of them occur in middle-aged patients who are injured during sports activities.
ANATOMY
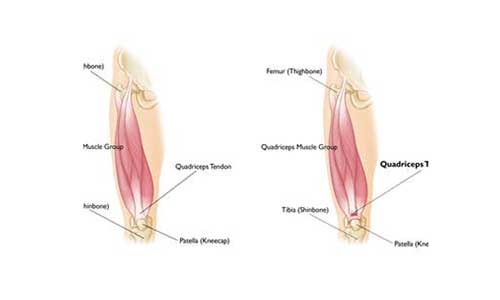
The 4 muscles of the quadriceps muscle group converge just above the patella to form the quadriceps tendon. The quadriceps tendon attaches the muscles mentioned above to the patella. The patella is attached to the tibia via the patellar tendon. Working together (quadriceps, quadriceps tendon and patellar tendon) extend the knee.
DESCRIPTION
Quadriceps tendon ruptures can be complete or partial.
Partial rupture: Many ruptures are not extended in the entire length of the tendon. For example, when a rope is stretched, some of its fibers are stretched too much but the rope remains intact, in the sense that it is not broken.
Complete rupture: A complete rupture cuts the tendon into 2 pieces. When the quadriceps tendon is completely ruptured, it is completely detached from the patella and knee extension cannot be performed.
ETIOLOGY
Injury: A tendon is ruptured when a large force is applied to the knee with the leg stretched and the knee partially bent. For example, an abrupt landing after a rebound in basketball may lead to a rupture. The landing force is too large for the tendon and it gets ruptured. Rupture can also occur after a fall, or after a direct force on the anterior surface of the knee, or even due to trauma.
Tendon atrophy: A weak quadriceps tendon is more likely to rupture. Several causes lead to tendon weakness.
Tendonitis: Chronic inflammation of the quadriceps tendon weakens it and can even cause minor ruptures. Quadriceps tendonitis is more common in runners and athletes who engage in activities that involve jumping.
Chronic disease: Tendon atrophy can be caused by pathological conditions that reduce blood flow to the tendon. These are:
- Chronic kidney failure
- Hyperparathyroidism
- Gout
- Leukemia
- Rheumatoid arthritis
- Systemic lupus erythematosus
- Diabetes Mellitus
- Infection
- Metabolic Disease
Use of Steroids: The use of steroids and anabolic–androgenic steroids as medication has been found to lead to atrophy and weakness of the musculoskeletal system.
Fluoroquinolones: This particular class of antibiotics has been associated with an increased risk of quadriceps tendon rupture.
Immobilization: When the patient is bedridden for a certain period of time, the muscles are atrophied and their risk of rupture increases.
Surgery: Although rare, quadriceps tendon ruptures can be caused after a knee surgery or even after a dislocation.
SYMPTOMATOLOGY
When the tendon of the quadriceps is ruptured there is often a sense of tear-cutting or a “click” that the patient feels. In most cases pain and edema follow and the patient is unable to extend the knee. Additional symptoms are:
- A gap in the upper part of the patella where the quadriceps tendon was ruptured
- Bruising
- Local sensitivity
- The knee can move towards the knee because it is no longer anchored
- Difficulty in walking because the knee is unstable or loose
CLINICAL EXAMINATION
The treating physician will request information on the patient’s general health status by obtaining a detailed medical history. Questions may include:
- Whether or not the patient has previously had a similar or other knee injury
- Whether or not the patient suffers from tendonitis of the tendon of the quadriceps
- Whether or not there are any medical problems that may predispose to a knee or quadriceps tendon injury
- Whether or not the patient has previously had knee surgery
After completing the above procedure, the physician examines the patient’s knee in detail. To determine the exact cause of the symptoms, the Orthopedist will check the knee extended. Although this part of the test is painful, it is important in the diagnosis of a rupture in the quadriceps tendon.
After completing the above procedure, the Orthopedist will examine the knee in detail. To determine the exact cause of the condition, the treating physician will check the joint extended. Although this part of the examination is painful, it is very important in the diagnosis of a patellar tendon rupture.

DIAGNOSTIC EXAMINATIONS
To confirm the diagnosis, the physician will order a series of tests, such as simple radiographs or magnetic resonance imaging.
X-rays: The patella moves out of position when the patellar tendon is ruptured. This is very evident in the lateral X-rays of the knee. Complete ruptures can only be confirmed with these shots.
Magnetic resonance imaging (MRI): This method can provide better images of soft tissues, such as the quadriceps tendon. Magnetic resonance imaging will depict the extent and morphology of the rupture. Often magnetic resonance imaging is required to exclude injuries with similar symptomatology.

TREATMENT
Conservative treatment: Very small and partial ruptures respond very well to conservative treatment, which usually involves the use of splints and physiotherapy.
Immobilization: The treating physician may recommend the use of a splint for 3-6 months, which will keep the knee extended to assist in the healing procedure. The patient will probably need crutches to avoid charging the affected leg.
Physiotherapy: When the initial pain and edema subsides, physiotherapy can begin. Specific exercises can restore muscle strength and range of motion.
During splint use, the treating physician may suggest exercises to strengthen the quadriceps. Knee lifts are often recommended with the lower extremity extended. Over time, the physician will unlock the splint to allow wider range of motion. Gradual strengthening exercises will be recommended during healing.
Surgery: Many patients need to undergo surgery to restore knee function. The surgical treatment consists of suturing the tendon. If it is a complete rupture of the tendon or a partial rupture of a degenerated and atrophic tendon, the Orthopedist must propose surgical treatment. This will depend on the patient’s age and level of activity.
Patients who undergo surgery report better results when surgery is performed as soon as possible after the injury. Quick treatment prevents tendon scarring and shrinkage.
Hospital Stay: Although the quadriceps tendon rupture suturing can be performed as a one-day outpatient procedure, it is preferred that the patient stays in the hospital for one night. This of course depends on the treating physician and whether the surgery was performed under regional anesthesia (epidural) or under general anesthesia.
Surgical Procedure: The tendons are restored by using sutures placed on the tendon, as well as on the bone, at its origin, with the surgeon properly adjusting the applied tension. This will restore the rupture to the pre-injury condition.

Newer technique: A new development in the field of repairing this type of injury is the use of anchors. Because it is a completely new technique, there is still not much data on its effectiveness.
In order to hold the patella in place and prevent the tendency of the materials to break, many surgeons use other materials to strengthen the suture, such as wires, which however need to be removed in a second surgery in the future.
If the tendon is significantly shortened prior to surgery, then reattachment can be a difficult task. In this case, a tendon graft may be used to lengthen the tendon.
Complications: The most common complications of patellar tendon repair include weakness and loss of movement. New ruptures can occur and the fixed tendon can be detached again. In addition, the position of the patella may be different after surgery. As with any surgery, other possible complications are: inflammation, trauma re-opening, thrombosis or even anesthesia problems.
Remedy: Some type of analgesia will be required after surgery, including ice pads and analgesics. Two weeks after surgery, the sutures will be removed by the treating physician. In all likelihood, the knee will be protected by a splint. Initially, the doctor may recommend only minimal contact and no load-charging activities.
Over time, the orthopedist can loosen the splint to allow wider range of motion. Strengthening exercises will be added later to the original plan. Complete recovery takes about 6 months, although some patients claim that it took them 12 months to reach their desired goal. The exact time to repair a quadriceps tendon rupture is individualized to the patient, always in relation to the type of the ruptured tendon, surgical repair, concomitant medical problems and finally the patient’s needs.
RESULTS
Most patients return to pre-injury levels in terms of lifestyle habits. There are many who report knee stiffness, while most regain full range of motion. In case of an athlete, the surgeon must examine the injured knee before allowing the patient to return to sporting activities. The goal is for the affected leg to reach 85-90% of normal functionality. In addition to all of the above, the treating physician will work to restore balance, endurance, and check for persistent edema.
