The synovial bursas are small gelatinous sacs found in many parts of the body, such as the shoulder, the elbow, the hip, the knee, the heel and elsewhere.
They contain a small amount of liquid, located among soft tissues and help to reduce friction. Like all synovial sacs, the prepatellar bursa serves to reduce friction between adjacent anatomical formations.
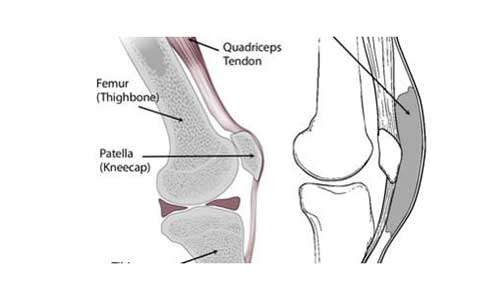
Pre-patellar bursitis is an inflammation of the bursa on the anterior surface of the knee, between the patella and the skin. It occurs when the bursa becomes irritated and produces a greater amount of fluid causing edema and pressure to the surrounding tissues.
ETIOLOGY
Pre-patellar bursitis is caused by continuous pressure or the microcirculation of the knee area after repeated kneeling. Some occupations such as builders, plumbers, miners or even housewives are at greater risk of developing pre-patellar bursitis.
Direct knee injury can also lead to pre-patellar bursitis. Athletes involved in so-called “contact sports” such as football, basketball, wrestling and more are at greater risk of developing this condition.
Another category of people with an increased risk of pre-patellar bursitis is patients with rheumatoid arthritis or gout.
Finally, pre-patellar bursitis can occur after a bacterial infection. It involves a trauma that creates contact between the bursa and the environment that can cause infection.
SYMPTOMS
- Pain during movement or exercise that usually subsides during night rest
- Swelling on the anterior surface of the knee
- Sensitivity and temperature change during skin palpation
- Bursitis after bacterial infection can cause fluid or cyst outflow (as there is trauma in the affected area)
CLINICAL EXAMINATION
Individual Medical History and Physical Examination:
The orthopedist asks details about the patient’s symptoms, such as the severity of pain, its duration, and the potential risk factors for the occurrence of pre-patellar bursitis. In addition, the physician should search for symptoms of infection such as fever and chills, since microbial infection requires another treatment plan.
During physical examination, the Orthopedist reviews the knee and compares it with the healthy one. During palpation, he looks for signs of sensitivity and evaluates the range of motion of the joint.
EXAMINATION
Radiographs: They are not diagnostic but can rule out a possible fracture of the patella
Other Imaging Tests: Computed tomography (CT) and MRI (magnetic resonance imaging) may describe other possible soft tissue lesions.
Punctuation: In suspicion of microbial infection, the physician uses a needle to get a sample of fluid from the bursa for laboratory analysis.
TREATMENT
Usually pre-patellar folliculitis is treated conservatively (non-surgically) if it is not due to a microbial infection.
- Rest: Avoiding movements and exercises that exacerbate symptoms.
- Ice therapy: Apply ice to the joint 3 or 4 times a day for 20 minutes each. Combined with rest reduces edema.
- Elevation of the leg, especially during the first few days to reduce edema.
- Medication: Anti-inflammatory drugs such as naproxen or ibuprofen can relieve pain and edema.
If pain and edema do not recede by these means, the orthopedist may decide to puncture the joint and remove the fluid. In addition, he may inject corticosteroid drugs (cortisone). Infectious bursitis is initially treated with antibiotics, but surgical drainage of the follicle is often needed. If the edema persists, the orthopedist may recommend surgical removal of the bursa. After surgery, the patient returns to his/her daily activities within weeks.
PREVENTION
The patient can help prevent pre-patellar bursitis by following these simple recommendations:
- Wear knee protectors for athletes or professionals who kneel at work.
- Rest on a regular basis with frequent breaks and knee extensions. Avoid abrupt knee movements or exercises.
- Elevation of legs and ice therapy after a long tiring day.
