
WHAT IS THE ROLE OF INTERVERTEBRAL DISCS?
Intervertebral discs play an important role in the spine. They serve as shock absorbers between the vertebrae. They support the weight of the human body and allow a wide range of motions in all directions.
The intervertebral disc consists of a central nucleus pulposus. It also contains a viscous gel consisting of proteins, polysaccharides, minimal chondrocytes and a large amount of water (88%). It is surrounded by concentric layers of fibrous tissue and collagen, the fibrous ring. When the physicochemical state of the nucleus pulposus is normal, (usually at younger ages) the disc can withstand heavy loads without particular problems.
Over time, the nucleus pulposus and fibrous ring lose much of their properties. For this reason, even small forces and loads can cause the fibrous ring to break and leak. Depending on the location of the damage, pressure can cause pain in the waist (lumbar region), as well as pain and neurological symptoms in the lower extremities.
The symptoms of the intervertebral disc hernia usually begin without any particular traumatic event. Incidents like this are lifting some light weight or turning the waist steeply. It is a common disorder of the musculoskeletal system. It is most commonly found in the lumbar spine between 35 and 50 years of age. At this age, the disc has already undergone significant degenerative changes. In contrast, vertebral stenosis is more commonly found in people over 60 years of age.
DEGENERATION AND INTERVERTEBRAL DISC HERNIA
Due to the natural process of aging and deterioration, the discs lose much of their content. Under normal conditions it provides them with elasticity and durability. As a result, the disks become harder and flat. This process, also known as degeneration, begins at an early age. It is often depicted early on imaging examinations (X-rays, CT scans and MRI).
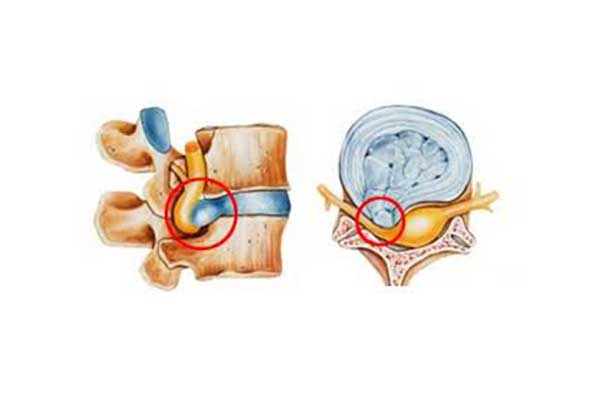
When repetitive axial pressure is applied to the spine, the disc and especially the fibrous ring may rupture or crack. In the lumbar spine, the protrusion of the disc can lead to pressure effects on the closest root of the spinal nerves. In addition, the leaking material can irritate the nerve. This can cause local inflammation. The result is an acute feeling of pain that reflects from the lumbar spine to the buttocks and lower limbs. Finally, it is important to note that disc degeneration (discitis) is not necessarily a progressive condition per se. It does not always lead to an intervertebral disc hernia.
There are many terms used to describe the various pathological conditions of the intervertebral disc and the associated pain. Some of them are “herniated disk” and ” intervertebral disc hernia” which are used indiscriminately.
Unfortunately, healthcare professionals do not agree with the exact definition of these clinical cases. At the same time, patients feel confused by hearing different terms about the same problem.
Instead of dealing with the exact terms that describe the problem, it is more useful to get a clear picture of the exact medical diagnosis. A medical diagnosis determines the true cause of pain in the lumbar area and lower extremities of the patient.
In order to diagnose, the Orthopedist follows three specific steps:
- Get medical history
- Complete physical examination
- One or more diagnostic tests (if needed).

SYMPTOMS OF INTERVERTEBRAL DISC HERNIA
While disc herniation in the lumbar spine can be extremely painful, for most patients the symptoms do not last for long. About 90% of people who experience symptoms of lumbar disc disease recover within six weeks, even without medical care.
It is believed that the symptoms mainly arise for three reasons:
- The body’s defense attacks the material of the hernia as foreign body. It thus shrinks its size, thereby gradually depressing the root of the compressed nerve.
- Over time, the cystic nucleus dehydrates in the context of aging, reducing its overall volume. This makes it less likely to expand and compress a nerve or the spinal cord.
- Spine stretch exercises can move the disc material away from the nerve roots or even into the fibrous ring again. But this is a theory that is the subject of debate in the medical community.
It is generally believed that symptoms improve because the smaller the size of the disc material, the less is the chance of nerve irritation. At the same time a large part of the disc is absorbed. Although the intervertebral disc hernia requires attention when it is painful for the patient, it has been found that many times the visual appearance of a hernia is not necessarily accompanied by pain or other symptoms.
COMMON HERNIATED DISK SYMPTOMS
As mentioned, it is common for a disc herniation to cause pressure effects on a nearby nerve, causing pain that reflects on the entire length of the nerve distribution (i.e., the area that is innervated by that nerve).
The hernia of a lumbar intervertebral disc is the most common cause of sciatica, i.e. pain and tenderness at the back of the lower limb. Some of the most common features are:
- Lower extremity pain: Usually the intensity of pain in the leg is greater than that in the lumbar area. If pain involves the sciatic nerve it is referred to as sciatica.
- Neurological symptoms in the lower extremity: Hypersensitivity, anesthesia and weakness are some of the symptoms that the patient may report.
- Symptoms with changes in localization: Depending on the size of the hernia and its location in the vertebral cavity, symptoms may include the lumbar spine, the buttocks, as well as the anterior or posterior part of the femur, tibia or foot, while typically it affects only one side of the body.
- Foot drop: Sometimes a large hernia can squeeze the nerve to the point that it causes weakness-paralysis of specific muscles (anterior tibial muscle) that promote dorsal flexion of the foot, leading to stressful nerve palsy.
- Low back pain: Pain in the waist (lumbar spine) occurs in most cases, but not always, and is accompanied by stiffness. It subsides after a few days (bed rest).
- Pain exacerbated by movement and certain postures: Pain can worsen after prolonged standing or walking, sneezing, or even intense laughter.
TWO MAIN CAUSES OF PAIN: NERVE PRESSURE (NERVE ROOT INFLAMMATION) AND DISC PAIN
Two terms are used to identify the cause that may cause pain in the lumbar spine and affect the intervertebral disc:
NERVE ROOT INFLAMMATION
When the patient suffers from a symptomatic herniation of the intervertebral disc, the disc itself is not painful. On the contrary, the material (nucleus pulposus) that collapses or leaks from inside the disc presses and irritates the closest root of the nerve exiting the spinal cord. This injury produces a feeling of pain called radical pain. Beyond the lumbar region (back pain) it also reflects on other parts of the body and especially the lower extremities. In the case of the nerve roots that make up the sciatic nerve, it is called sciatica.
DISC PAIN
If the patient suffers from significant degeneration of the intervertebral disc, without disc herniation, then the pain is located in the specific area and is exclusively due to degeneration of the disc without reflection in the lower extremities (axial pain).
Any of the above symptoms may affect the cervical, thoracic, or lumbar spine. However, in the majority of cases they are located in the lumbar spine (‘middle’). This is because it absorbs most of the load that the spine receives on a daily basis.
It should be borne in mind that the term “disc herniation” or “degenerative disc” refers to imaging findings of X-rays, CTs or MRIs. Although very important, they are not enough to determine the exact cause of the pain. On the contrary, the clinical picture and physical examination of the patient by the Orthopedist will finalize any suspicion and lead to an accurate diagnosis.
RARE BUT DANGEROUS SYMPTOMS – CAUDA EQUINA SYNDROME
The loss of bladder control (urinary incontinence) or intestine control (fecal incontinence), as well as numbness in the back of both thighs with concomitant weakness in the lower limbs are symptoms of the Cauda Equina syndrome. This is a serious and urgent pathological condition. It is caused by a large hernia that presses on the nerve roots coming out of the medullary cone (Cauda Equina). The patient must be treated surgically within 48 hours in an effort to reverse the neurological damage.
DIAGNOSIS
Clinical diagnosis follows a specific series that includes:
- The medical history
- The physical examination
- The imaging examinations
MEDICAL HISTORY
Patients presented with the orthopedic symptoms mentioned above should be asked about:
- The type of pain. The patient is asked to describe the features of pain, including the location and the activities that trigger it.
- Concomitant health problems, such as Osteoporosis
- Information on the patient’s work and daily living.
- Family history
- Finally, any history of anxiety disorder or depression should be discussed with the treating physician.
CLINICAL EXAMINATION
It is the most important step in the diagnosis and involves the observation of the patient’s movements, as well as palpation in combination with some special tests.
More specifically:
- Neurological Examination: In order determine if there is a particular neurological defect, the Orthopedist examines the lower limbs for signs of hypersensitivity, swelling or weakness. The patient is usually asked to walk on the toes and the heels, while finally controlling the reflexes of the lower limbs.
- Range of motion: The patient is asked to bend and extend his or her waist as far as the pain allows.
- Lasegue Test: With the patient in a supine position and the knees stretched, the Orthopedic bends the legs and triggers pain in the waist (lumbar spine) usually between 30 ° and 70 °.
- Complete neurovascular examination of both lower extremities
- Palpation of the lumbar area
- Observation of the patient’s gait
If none of the above symptoms are observed and the level of pain is tolerated by the patient, further imaging is often required and a re-examination is planned.
IMAGING EXAMINATIONS
Imaging is performed on the one hand to rule out some of the rarer causes of back pain, such as fractures, tumors and infections. On the other hand, it is also used to better describe and confirm the findings of the preceding clinical examinations.
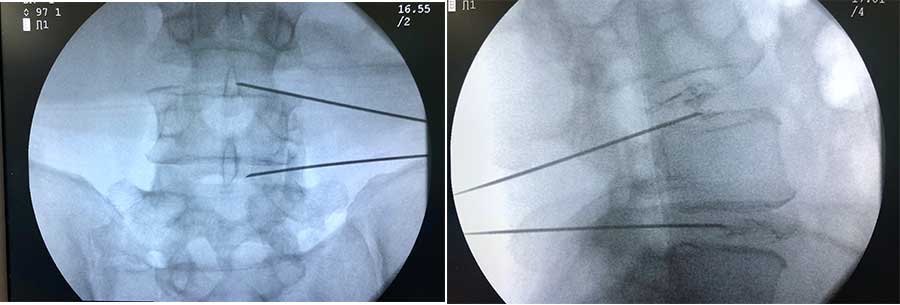
- Radiographs: To rule out possible fractures (e.g. in patients with osteoporosis or a history of trauma) tumors or infections.
- Magnetic Resonance Imaging: It usually provides the most detailed information on whether or not a herniated disc is present, its location and size, as well as the compressive effects it causes. It is often performed for preoperative planning. It helps to rule out spinal stenosis.
- Computed tomography: Where magnetic resonance imaging is contraindicated.
- Myelogram or CT Myelography (CT): A contrast agent is used to visualize the spinal cord and spinal nerves. It may provide detailed information on the herniated disk but it is considered an invasive examination.
- Electromyogram: It can identify the affected nerve root.

TREATMENT
CONSERVATIVE TREATMENT
In the majority of cases of lumbar disc herniation the symptoms subside within six weeks. For this reason, conservative (non-surgical) treatment is initially recommended, except in cases where the symptoms include severe neurological problems.
PAIN CONTROL
The control of severe pain is an urgent need when the first symptoms arise. Initial options include:
Medication: Non-steroidal anti-inflammatory drugs (NSAIDs) are a class of medicines that greatly relieve the patient. In addition, some muscle relaxant medications can reduce muscle spasm in the lumbar spine.
Warm-cold pads: They help relieve painful muscle spasms after the first 48 hours.
Bedding: Bed rest can relieve the patient but is only recommended for the first few days. Prolongation can lead to further stiffness. After the first few days it is recommended to avoid heavy manual labor and several rest breaks.
ADDITIONAL TREATMENTS
Physiotherapy: It is important to teach the patient some targeted spinal cord exercises in the recovery phase. In addition, the program can teach the patient safer ways to perform their normal daily activities.
Epidural infusion of steroids: It may provide long-term symptom relief and relieve the patient. However, it often does not resolve the problem and patients’ symptoms relapse.
Finally, the methods of acupuncture (FDA approved) and chiropractic are also recommended, which may be useful to the patient but only under specific indications for a limited number of patients. The patients should consult their orthopedist first for the diagnosis and exclusion of neurological deficits, as well as for treatment which may include well-known conservative and surgical methods.
When the pain and other symptoms persist and do not subside after a period of six weeks, then surgery is recommended to the patient. The intervertebral disc hernia in the lumbar spine is the most common cause of spine surgery in adults.
Surgery can be recommended if:
- The patient reports severe pain that does not allow him/her to maintain a normal level in daily activities, such as standing up and walking.
- Loss of bladder or bowel control (both symptoms being indicative of emergency surgery within 48 hours and not six weeks).
- Patient does not benefit from conservative treatment (NSAIDs, physiotherapy)
- The patient is experiencing progressively deterioration of neurological symptoms, such as weakness in the legs and/or numbness.
- In some cases (as mentioned) surgery may be recommended much earlier than six weeks.
LUMBAR MICRODISCECTOMY
In lumbar microdiscectomy, a small portion of the bone is excised above the nerve root along with much of the disc material that presses and irritates it, providing more space. Through a small incision, a “window” opens to the spine about three by four inches in diameter. Anything that can cause compressive effects on the nerve root is removed through this space.
More specifically:
- A small incision is performed about 3-4 cm in the midline of the spine at the height of the disc in the lumbar spine.
- The erector spinae are lifted and removed from the lamina of the vertebra. Since these muscles are vertical, it is recommended that they are removed and not intersected.
- The surgeon enters the spinal cord by removing a small portion of the ligamentum flavum. With the help of a surgical microscope, the surgeon can remove all those tissues (osteophytes, disc material) around the nerve root.
- Often a small part of the facet joint is removed to facilitate access to the nerve root and to increase the space around the nerve.
- The nerve root is then moved away with subtle manipulations and the disc material that puts pressure on it is removed.
- Since most of the joints, ligaments and muscles have remained intact, microdiscectomy does not alter the mechanical structure of the lumbar spine.
In general, the improvement of the patient’s symptoms due to intervertebral disc hernia is evident in the first six to twelve weeks. As long as the pain is tolerable and the patient is able to function satisfactorily, it is usually preferable to delay the operation for a short period of time to assess whether the symptoms will subside with conservative treatment or not.
If pain and other lower extremity symptoms do not recede with conservative treatment, then the minimally invasive method of microdiscectomy mentioned above is indicated.
Emergency surgery is necessary in cases of cauda equina syndrome or progressively worsening neurological deficits. Finally, severe pain in the lower extremity may also be an indication for surgery.
In conclusion, microdiscectomy is recommended in patients:
With pain lasting longer than six weeks not treated with conservative treatment (NSAIDs, Physiotherapy). However, the results of surgery are best when patients undergo surgery three to six months after the onset of symptoms.
SUCCESS RATES
The success rate for the minimally invasive method of microdiscectomy is about 90-95%, while 5-10% of patients will develop a herniated disc again at some point in their lives.
Recurrence may be observed immediately after surgery or many years later. However, it is most commonly observed within the first three months after surgery. In the case of relapse, the revision with the microdiscectomy method is equally successful. However, after a relapse, the patient is at greater risk of further relapses.
