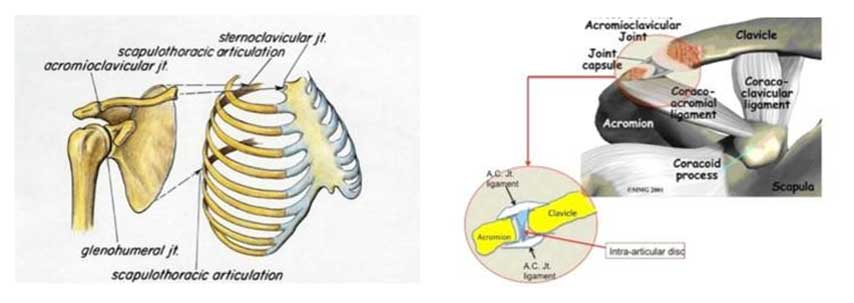
The injuries of the acromioclavicular joint occur in the acromioclavicular joint, which is located in the anatomical region of the shoulder and constitutes the connection between the distal end of the clavicle and the scapula, as the acromion is an anatomical part of the scapula and constitutes the palpable bone surface of the shoulder.
The acromion is attached to the clavicle by means of strong ligaments, the upper and lower acromioclavicular ligament, and contains an intra-articular cartilage disc that acts as a suspension (“or as a pillow”).
This is an important joint as it connects the shoulder to the rest of the body and is a source of severe pain after injury.
What Causes Pain in Injuries of the Acromioclavicular Joint?
Under normal conditions, the rigid cartilage disc between the acromion and the clavicle acts as a suspension that allows free movement between the two bones when the shoulder moves.
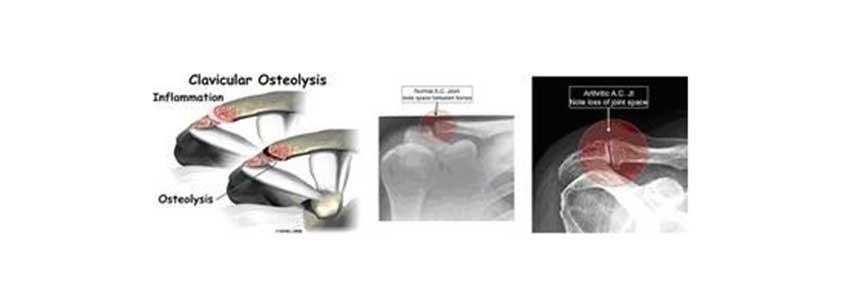
However, sometimes this disc can degenerate over the years, after repeated shoulder lifts or weight lifting, or it can be injured after a fall on an extended upper limb.
This has as a consequence pain and some mechanical symptoms, creating a “click” or “clench” sensation.
The inflammation caused may lead to osteolysis and degeneration of the joint, a pathological condition often observed in weightlifters.
In some cases the pain may be due to osteoarthritic lesions that are part of a normal aging process, but may be the result of injury or repetitive articular loads.
In these cases, the condition is called post-traumatic arthritis.
Causes – How do injuries of the acromioclavicular joint occur?
The acromioclavicular joint is very often subject to injuries.
In many cases, the mechanism of injury involves a fall on the shoulder in extended position or immediate injury of the area.
Team contact sports (soccer, basketball, jockey, etc.) are mainly the ones to blame for injuries of the acromioclavicular joint.
As mentioned above, the acromioclavicular joint is reinforced by strong ligaments which, in combination with the coracoclavicular and acromioclavicular ligaments, provide stability to the shoulder.
These ligaments can:
- Get injured
- Stretch (sprain)
- Undergo partial ligament tear
- Undergo complete ligament tear
leading to dislocation or separation – distension of the acromioclavicular joint.
All these injuries are classified as follows:
Grade I: Sprain, the acromioclavicular joint ligament is intact
Grade II: Acromioclavicular joint ligament rupture, sprain of the coracoclavicular ligament
Grade III: Rupture of both ligaments (acromioclavicular and coracoclavicular ligament). The acromioclavicular joint is dislocated
Grade IV: III with the clavicle directed backwards to/through the trapezoidal muscle
Grade V: III with the clavicle directed upwards
Grade VI: III with the clavicle directed downwards
After the injury, severe pain develops either due to the extension or rupture of the ligaments or due to injury of the intra-articular disc. In the event of a rupture, this can lead to dislocation of the acromioclavicular joint with obvious deformation, palpable clavicle and inability of shoulder movement.
This is due to the loss of normal support of the arm and shoulder in general, which gives the impression that the peripheral clavicle protrudes. Patients with distension of the acromioclavicular joint can develop acute or chronic pain and some degree of shoulder instability.

How are the injuries of the acromioclavicular joint treated?
The pain caused by either arthritic lesions or osteolysis can be treated in many ways.
Conservative treatment is the first approach to the problem, and includes:
- Rest
- Use of a splint
- Modification of daily activities
- Anti-inflammatory drugs
- Use of cold or hot pads
- Physical therapy (ultrasound)
When conservative treatment fails to relieve the patient from pain, intra-articular injection of corticosteroids and topical anesthesia may be useful.
On the one hand, it reduces the inflammatory response and drastically relieves the pain, and on the other, it confirms the diagnosis of joint injury.
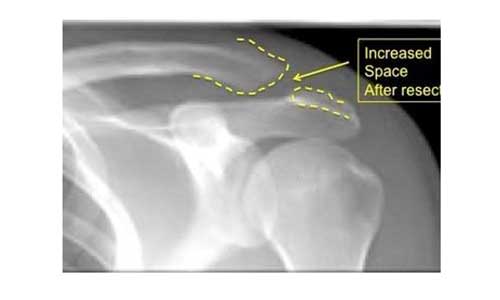
In cases where pain continues to affect a patient’s quality of life despite conservative treatment, surgery becomes a valid option.
In this surgical procedure a part of the clavicle and the acromion along with the articular disc in order to create space so that there is no irritation.
The procedure can be performed arthroscopically or in open surgery, since both are equally effective.
How to treat an acromioclavicular joint separation-distension?
The treatment of the distension of the acromioclavicular joint is controversial.
For most cases of acromioclavicular joint distension, conservative treatment is an acceptable method of management.
This applies to 1st and 2nd degree injuries.
3rd degree injuries can be treated conservatively with a good level of pain relief if the patient is willing to accept the projection of the clavicle.
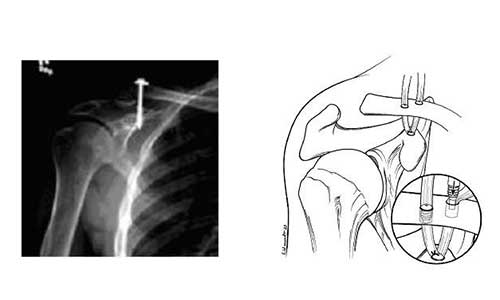
However, some surgeons suggest immediate surgical fixation using a screw or suture.
To date, however, there is no clinical experience in the literature to support this approach.
In 4th and 5th grade injuries with severe distension of the acromioclavicular joint, there is a greater chance of pain and limited functionality with conservative treatment only, and surgery is the most reasonable solution.
When the dimension of the acromioclavicular joint is chronic (more than a few months), the joint is reconstructed and restored using:
- Topical ligaments (autografts)
- Cadaveric tendons (allograft) in combination with strong sutures
Many surgeons now follow the second option (allografts) as they provide stronger local reconstruction of the articular joints. Whatever graft is used, surgery can be performed either by a combination of arthroscopic and open surgery or by a completely open surgery.
Recovery
AFTER ARTHROSCOPIC OR OPEN-SURGERY REMOVAL OF THE DISTAL END OF THE CLAVICLE
After the operation, the patient usually is discharged from hospital on the same day, wearing a suspension envelope-type splint.
During the first two days the patient may use cold pads to relieve the pain.
Then the suspension can be removed and the patient begins daily activities such as:
- Washing
- Dressing
- Driving
- Other daily activities
Depending on the case, the orthopedist will provide more specific instructions regarding the patient’s recovery and return to their daily and sporting activities.
AFTER RECOVERY – RECONSTRUCTION OF THE ACROMIOCLAVICULAR JOINT
And in this operation, the patient leaves the hospital on the same day of surgery, wearing a suspension envelope-type splint.
During the first few days, along with painkillers, cold pads may be used to avoid edema and pain.
The suspension splint will be worn for a period of 6 weeks so that the joint can heal.
The suspension splint can be removed during daytime (e.g. during bath time), but under no circumstances the operated limb may be used during the first 6 weeks.
