The term fracture refers to a broken bone. Fractures of the femur located just above the knee are called distal femur fractures. Such fractures are diagnosed either in elderly people with osteoporotic bones or in younger people that have suffered high energy injuries, such as in traffic accidents. In both cases the fracture can be comminuted (several bone segments) and extend into the knee joint.

Anatomy
The knee is the largest loaded joint in the body. The femur is located at the top of the knee joint and the tibia is just below it, supporting the lower part of the joint. The tip of the femur is covered by a smooth cartilage that helps in sliding. This cartilage helps to protect and dampen the knee vibrations, when flexion-extension movements are performed.

Strong muscles in the anterior surface of the knee (quadriceps), as well as in the posterior surface (biceps) support the knee and allow flexion-extension movements.

Description
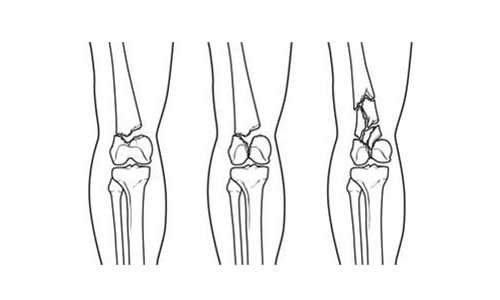
Fractures of the distal femur vary. The bone can be broken laterally (transverse fracture) or in several pieces (comminuted fracture). Sometimes such fractures extend to the knee joint and divide the surface of the knee into several pieces. Such fractures are called intraarticular. Given the fact that they damage the articular surface of the bone, intra-articular fractures are more difficult to handle.
Fractures of the distal femur may be closed (in the sense that the bone does not come in contact with the surrounding environment) or may be open. An open fracture occurs when the bone breaks in such a way that the bones penetrate the skin or in such a way that the wound reaches such a depth that it contacts the bone. Open fractures usually involve greater damage to adjacent soft tissues such as tendons, muscles and ligaments.
They take longer to heal and are usually accompanied by more complications. When the distal femur is fractured, the quadriceps and biceps muscles contract and shorten, making it difficult to maintain fracture alignment in the splint.

Etiology
Fractures of the distal femur usually occur in two categories of patients: Young people (under 50 years of age) and older people.
- Fractures of the distal femur in younger patients usually occur after high-energy injuries, such as falls from height or traffic accidents. Because of the mechanism of injury, many patients suffer concomitant injuries, often in the head, chest, abdomen, pelvis, spine and elsewhere in the body.
- Older people with distal femur fractures usually have poor bone quality. With age, the bones lose bone density and become slowly weak and fragile (osteoporosis). Even a milder injury mechanism, such as a simple fall to the ground, can cause this kind of fracture. Although these patients may not have any other injuries, they may still have concomitant health problems such as cardiovascular, pulmonary, kidney disease or even diabetes mellitus.
Symptoms
The most common symptoms of distal femoral fractures are:
- Pain (Charging with weight is usually impossible)
- Edema and bruising
- Sensitivity to palpation
- Deformity; the knee may be dislocated and the leg may appear shorter and deformed. In many cases these symptoms can be located around the knee, but in many cases there may also be symptoms in the thigh area.
Clinical examination
It is important for the Orthopedist to know the conditions under which the injury occurred, for example, from what height the fall occurred. It is also important for the orthopedist to know if the patient has injured another part of the body or if he/she has other health problems such as diabetes. Finally, it is important for the physician to know if the patient is taking any medication regularly.
Subsequently, the orthopedist must proceed to a clinical examination.
- All possible injuries (head, chest, abdomen, pelvis, spine and other parts of the body) shall be estimated
- The skin around the fracture site shall be examined to evaluate whether or not it is an open fracture.
- Finally, the patient’s spinal nerve function shall be evaluated
Examination
Other examinations that assist in the diagnosis of the fracture are:
- Radiographs: The simplest and most common way to diagnose a fracture is to have an X-ray. In this way, the morphology of the fracture and its complexity will be revealed. In addition, in order to clarify that there are no other fractures, X-rays will be performed on both the hip and the ankle joint.
- Computed tomography: It will provide the transverse image of the bone, as well as information on the severity of the fracture. It will clarify whether the fracture extends into the joint and if so, how many bone fragments are present. This test greatly helps your physician design the most appropriate treatment method.
- Other tests should follow to rule out other injuries to the head, chest, abdomen, pelvis, spine and other parts of the body. Sometimes vascular integrity tests are also performed.

Treatment
Conservative treatment
Skeletal traction: This is a system of pulleys with weights and counter-weights to hold the lower parts together. A pin is inserted into the bone to hold the leg in place.
Splint: Various splints may hold the bones in their proper position until healing is achieved.
In many cases of fractures of the distal femur, however, a splint alone cannot properly align the fractured bone sections due to the shortened muscles that pull the bones out of position. Splint treatment is limited to those fractures that are two-pieced, firm and well-aligned. Also, splints may not be well-tolerated by patients. A very important parameter for patients with this type of fracture is the rapid mobilization, that is, to be able to self-serve as soon as possible after therapeutic intervention. The treatment that ensures quick mobilization, reduces the risk of stiffness and eliminates problems caused by prolonged bed rest (pressure ulcers and thrombosis) is the surgical one.
Because skeletal traction and splints do not allow for quick mobilization, they are less and less used today. The orthopedist will evaluate what the best therapeutic approach will be.

Surgical treatment
Due to the available methods nowadays and the newer materials used, surgical treatment is indicated even in older patients with osteoporosis.
Surgery planning:
Many fractures of the distal femur are not operated immediately unless they are open fractures. In open fractures, the bone comes into contact with the contaminated environment, which requires immediate wound healing and surgical cleaning. In most cases, the operating room may be delayed by one to three days for proper planning.
External Osteosynthesis:
If the soft molecules (muscles, skin) around the fracture are seriously injured, or if additional time is required for surgery due to other concomitant problems, then the Orthopedist may use an external osteosynthesis. In this case, metal pins and screws are inserted in the middle of the femur and tibia and attached to a frame outside the skin. This device is bone-stabilizing in an appropriate position until the surgery. When this is possible, the surgeon will remove the external osteosynthesis and proceed to internal osteosynthesis with plate and screws.
Internal Osteosynthesis:
The methods of internal osteosynthesis that most surgeons employ are:
Intramedullary Nailing: In this case a specially designed nail enters the bone marrow cavity. The nail passes through the broken pieces of bone and stabilizes them, thereby supporting and aligning them.
Plate-Screws: During this procedure, the bones are first aligned, that is, they are placed in their proper anatomical position and then, they are held together by specially designed metal screws and plates that adhere to the outer surface of the bone.
Both of these methods can be performed through larger or smaller incisions, depending on the type of fracture and the type of materials used by the surgeon.

In some extreme cases a fracture can be so complicated and the quality of the bone so poor to be restored that treatment involves removal of the bone fragments and replacement of the bone with knee prosthesis.

As the population ages and the number of total arthroplasty surgeries rises, a new phenomenon has emerged: The fracture of this type mentioned above in patients who have already undergone total knee arthroplasty (peri-prosthetic fractures). Such fractures are usually treated with rods or plates just like the rest fractures of the distal femur. In rare cases, the existing prosthesis is removed and replaced by an older or longer prosthesis. This procedure is called a revision and is performed when the joint is loose and there is not enough bone substrate of good quality.

Complications
To prevent complications, intravenous antibiotic treatment will be administered preoperatively. Anticoagulants will also be administered to prevent clot formation in the lower extremities. Finally, blood loss during surgery may require blood transfusions.

Rehabilitation
The fracture of the distal femur is a serious injury. It may take more than a year, depending on the general state of health, the type of fracture and the age of the patients, until they return to their daily activities.
Fast mobilization:
The orthopedist decides when is the best time for the patient to start moving his or her lower extremities to avoid knee stiffness. This depends on the healing state of the soft tissues, but also on the stability and healing process of the fracture. Rapid mobilization begins with passive mobilization to avoid stiffness. A physiotherapist gently moves the knee instead of the patient. If the fracture is comminuting, the healing period may be longer, resulting in a short delay in mobilization.
Weight-bearing
In order to avoid problems, it is necessary to follow the instructions of the Orthopedist in loading the leg with the weight of the patient. Whether or not surgery has been performed, the physician will prohibit weight-bearing until some degree of fracture healing is achieved (this can take up to 3 months). During this time, the patient will have to walk with the help of a walking stroller or crutches. Finally, a knee splint may be required for additional support.
The orthopedist shall request regular X-rays to assess the healing process and the proper alignment of the fractured bones. When the doctor decides that the healing process is well-advanced, he will encourage the patient to begin weight-charging. But even if the charging process begins, crutches may need to be used for assistance.
Rehabilitation – Recovery:
When the knee is allowed to be charged with weight, it is natural for the leg to be weak, unstable and stiff. Although this is expected to some extent, a patient-specific plan for restoring normal muscle strength, flexibility and movement should be discussed with the treating physician or physiotherapist.
The dedication to the physiotherapy-rehabilitation process plays a big role in how satisfactory the final result will be. For example, if the patient is a smoker he will be asked to quit, because smoking impedes the healing process. In order to assess the progress of the healing process, the patient should ask:
- Whether or not he/she is improved in self-service
- Whether or not he/she is improved on daily activities
- Whether or not the pain is reduced and the range of motion, stability and flexibility are increased at the same time.
The goals of recovery are set from scratch regardless of whether it takes up to a year until they are fully met.
Complications
Infection
The most up-to-date techniques used to treat these fractures have reduced to more than half the percentage rates of this complication. Less than 5% of patients present a post-operative infection nowadays. At the time of surgery, the orthopedist will administer antibiotic treatment to prevent infections.
Open fractures (with concurrent skin injury) as well as high-energy injuries (traffic accidents) are more likely to be infected. If the infection penetrates the deeper tissue layers, then it can affect the bone and the bone material that was used. Such an infection requires long-term antibiotic treatment and many surgeries to eradicate it.
Stiffness
Some degree of stiffness is always expected after a surgery. Quick mobilization after surgery is the best way to prevent stiffness. If, however, the fracture is healed but there is enough stiffness, then the Orthopedist can recommend an additional surgery to resolve the stiffness-causing adhesions.
Problems with fracture healing (Pseudoarticulation)
In some cases, bone healing may be too slow or may not happen at all. If any of the X-rays depicts osteosynthesis material (plates and screws) out of bone, then this is a sign of delayed healing. This can happen even though the fracture is optimally repaired and no mistake was performed. Open fractures as well as high energy injuries are more likely to suffer this complication. Fractures of this kind are also more susceptible to infections and this can cause non-healing problems.
To deal with this difficult situation, your Orthopedist may insert a bone graft and modify the osteosynthesis materials.
Post-traumatic knee osteoarthritis
Fractures of the distal femur extending into the articular surface of the knee disrupt the smooth construction of the articular cartilage. Since the knee is the largest loaded joint in the body, any injury that extends and involves part of the articular cartilage increases the likelihood of developing osteoarthritis of the knee at a later time. This type of arthritis is called post-traumatic arthritis and can be treated like osteoarthritis, i.e. physiotherapy, splints, medication and lifestyle modification. In severe situations, total knee arthroplasty is indicated.
Long-term results
Typically, it may take up to one year for the distal femur fractures to heal. Factors affecting fracture healing include:
- The severity of the initial injury. High-energy injuries or open fractures require more time to heal, especially if there is damage to soft tissues.
- The quality of the bone. When there is better bone quality, especially in young patients, then osteosynthesis is better maintained than in elderly patients to whom osteosynthesis may loosen. Newer techniques may reduce this chance, but the risk is real.
- The patient’s discipline and commitment to the rehabilitation-recovery program. Although this process is time-consuming, full dedication to the rehabilitation program and the instructions of the treating physician are required to achieve the best results.
The orthopedist assesses the progress of the recovery and the way the pain subsides and at the same time the return of the patient to daily activities is achieved.
Things to discuss with your doctor:
Is there a risk of me not healing adequately?
Do I have weak bones?
Do I need a splint?
What are the risks in the operating room?
What do I need to do to prevent clot formation?
Do I need blood transfusions?
Do I need a transplant? If so, where will it come from?
How long will I be on a sick leave?
When can I start bending my knee?
When can I put weight on my knee?
Will I get arthritis?
