Compartment syndrome is a painful pathological condition caused by an increase in pressure within the muscles at dangerous levels. This pressure can reduce blood flow and prevent nutrient transport and oxygenation of the soft tissues and especially of the nerves and muscle cells.
The compartment syndrome can be acute or chronic:
The acute compartment syndrome is a medical emergency and is usually the result of a serious injury. Untreated, it can lead to permanent damage to muscles and nerves.
The chronic compartment syndrome is usually caused by prolonged exercise (e.g. long distance runners) and is not an urgent medical condition. It is characterized by pain that is exacerbated by muscle activity.
ANATOMY
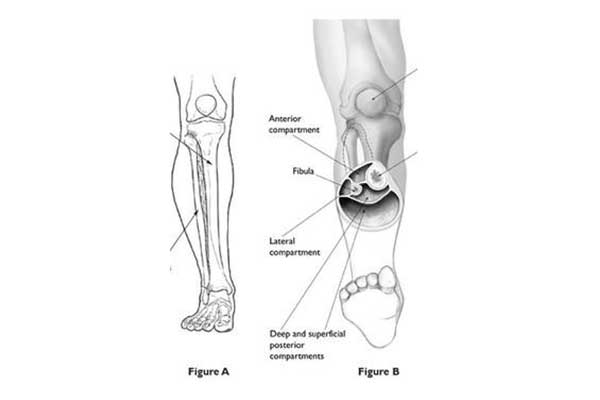
The compartments in the human body are defined as groups of muscles, nerves, and blood vessels in the lower and upper extremities, enclosed by a stiff and hard membrane called the fascia. The role of the fascia is to provide stability and, as such, it cannot be extended easily.
DESCRIPTION
The compartment syndrome develops due to edema in a compartment – mainly due to hematoma. Given that the fascia surrounding it is non-adherent, intra-compartmental pressure around the capillaries, nerves, and muscles increases, disrupting blood flow. Without constant supply of oxygen and nutrients, the nerves and muscles can be irreparably damaged.
In acute compartment syndrome, failure to decompress such anatomical space may result in tissue necrosis and permanent disability. On the contrary, in the chronic compartment syndrome, due to fatigue, no irreparable damage is described. Compartment syndrome most commonly occurs in the anterior compartment of the tibia, as well as in other parts of the body such as the arm, buttocks, hands, and feet.
ETIOLOGY
ACUTE COMPARTMENT SYNDROME
Acute compartment syndrome occurs after serious injuries such as traffic accidents or falls from height, usually involving serious injuries or fractures.
The causes for the development of compartment syndrome include:
- Fractures
- Injuries of soft tissue with significant bruising. This kind of injury can e.g. be the result of a bike crash, with tibia injury or a direct hit during sporting activities
- Crushing injuries
- Restoration of blood flow after prolonged inhibition due to vascular damage. Sometimes, blood flow can be interrupted by prolonged pressure during sleep. Normally, most healthy people are mobilized after developing transient ischemia while sleeping, but in cases of neurological disease or high consumption of alcohol or drugs, even compartment syndrome may occur.
- Anabolic Steroids
- Tight straps or splints. In suspicion of developing compartment syndrome they should be removed immediately.
CHRONIC COMPARTMENT SYNDROME
Excessive and prolonged effort during exercise can cause pain and swelling leading to chronic compartment syndrome. Athletes who engage in activities with repetitive movements such as running, cycling or swimming are likely – though rarely – to develop chronic compartment syndrome. The pain usually subsides when the exercise is ceased.
SYMPTOMS
ACUTE COMPARTMENT SYNDROME
- The classic symptom of compartment syndrome is pain, especially when the muscles in the compartment are stretched.
- The pain is more severe than would be expected from the injury itself and may be accompanied by hyposensitivity or paraesthesia of the area (numbness or “tingling” sensation) or even by a burning sensation.
- In particular, hypersensitivity and paralysis are symptoms that occur later on and are a sign of permanent tissue damage.
CHRONIC COMPARTMENT SYNDROME
The chronic compartment syndrome causes pain or cramping during exercise. Pain is relieved when exercise is ceased and most often it is related with the lower extremities.
Other common symptoms are:
- Hyposensitivity
- Difficulty in moving
- Visible muscle edema
CLINICAL EXAMINATION
ACUTE COMPARTMENT SYNDROME
This is an emergency. The patient must visit the emergency department of a hospital immediately. The physician, on suspicion of acute compartment syndrome, should measure intra-compartmental pressure to diagnose the syndrome.
CHRONIC COMPARTMENT SYNDROME
For the diagnosis of chronic compartment syndrome, the physician must rule out all other conditions that can mimic the aforementioned symptomatology, such as tendinitis. In addition the doctor may e.g. recommend radiological examination to exclude possible tibial fracture, due to fatigue.
For confirmation purposes, the doctor should measure the intra-compartmental pressure before and after exercise, while recording the differences.
TREATMENT
ACUTE COMPARTMENT SYNDROME
Acute compartment syndrome is an emergency that needs immediate surgical treatment. The Orthopedist with specific incisions will open the skin and the fascia surrounding the compartment. Most often, edema does not allow immediate skin closure. In this case, the surgical wound is closed during a second surgical operation, with or without the use of a skin graft.
CHRONIC COMPARTMENT SYNDROME
Conservative therapy:
Physiotherapy, orthopedic soles (footwear inserts) and anti-inflammatory drugs have dubious effects on relieving symptoms.
Symptoms usually subside with the modification of the patient’s daily and sporting activities. Low-intensity workout is the best choice. In addition, sometimes the symptoms get worse when exercising on certain ‘hard’ surfaces, such as on cement and non-artificial carpet or lawn and therefore the use of specific sports facilities is recommended to the patient.
Surgical treatment:
Due to the failure of conservative treatment, surgery is the final choice. In the same way that the acute compartment syndrome is treated, the fascia is opened to free up space for muscle movement. The conditions of the surgery are very different from those of the acute compartment syndrome and the surgical trauma is less, without the need for grafts.
